Featured answer
Here is the simple view of embryo transfer day by day after a day‑5 FET. DPT 1–3: no reliable signals. DPT 4–6: implantation may start. DPT 7–9: early hCG production; tests can still be negative. DPT 9–11: earliest sensible home tests. DPT 12–14: stronger positives if pregnant. Symptoms are unreliable. Call your clinic if you have red flags.
Introduction
The two‑week wait can feel loud. Every twinge seems to say something. This guide makes embryo transfer day by day simple. You will see the common DPT windows, how to time testing, and what symptoms are only side‑effects. We also link a “When to test after FET” explainer so you can plan calmly.
Embryo Transfer Day by Day: The Short Version
Why this matters
Blastocysts reach the uterus ready to attach. The window of implantation spans the first week after transfer. β‑hCG only starts after implantation, so early tests can be falsely negative. Set expectations and you lower stress (NICE 2019; RANZCOG 2023).
Quick DPT windows
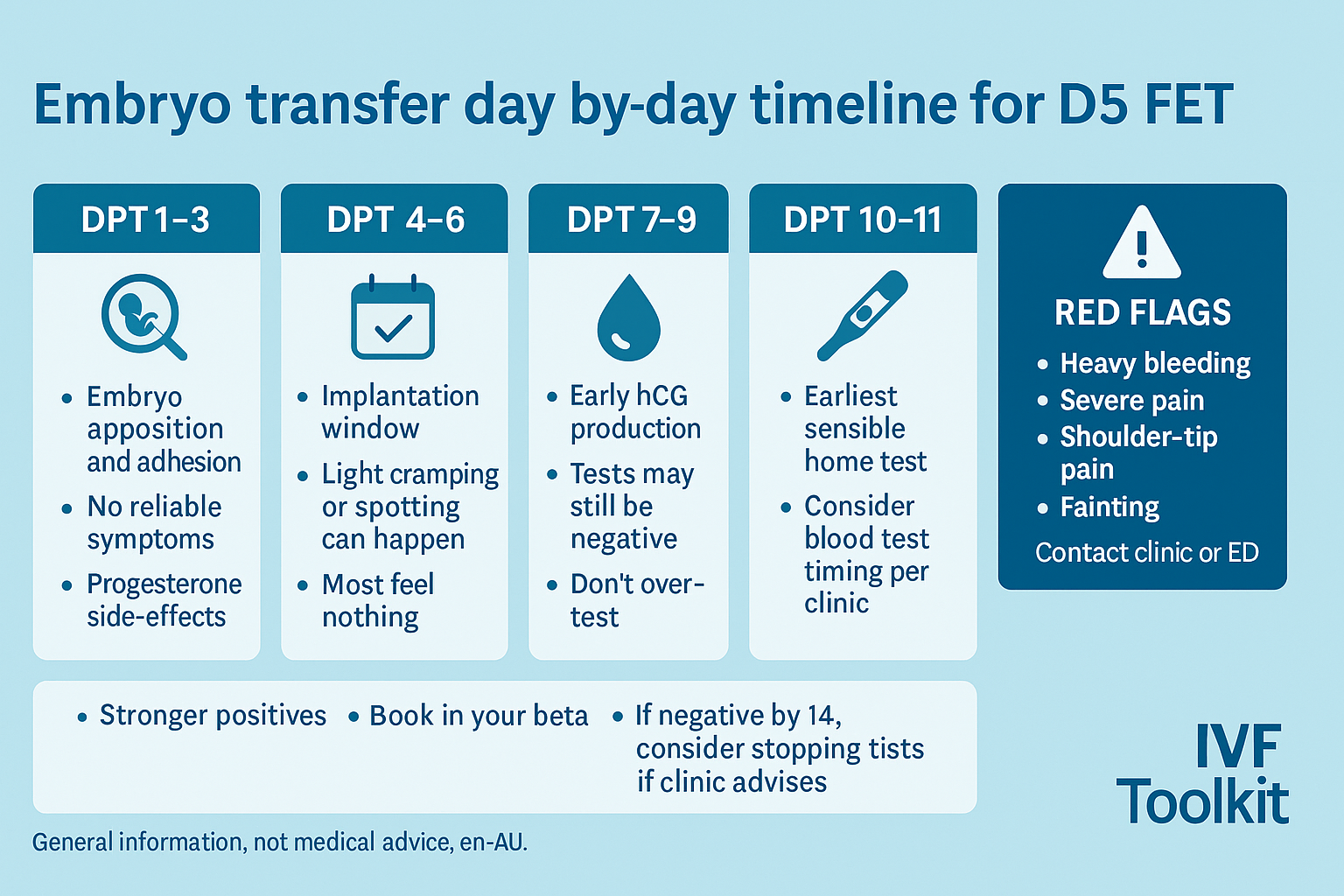
- DPT 1–3: settling in. No reliable signals.
- DPT 4–6: implantation window. Light cramps or spotting can occur but also happen with progesterone.
- DPT 7–9: early hCG. Home tests may still be negative.
- DPT 10–11: reasonable time to try a sensitive home test.
- DPT 12–14: stronger positives if pregnant. Plan bloods with your clinic.
Mistake to avoid
Reading tea leaves from symptoms. Progesterone can cause tender breasts, bloating, and mood changes regardless of outcome.
Evidence: Urine tests before 9–11 DPT often miss pregnancies after D5 transfer. Blood testing is more sensitive and should be timed with your clinic (RACGP 2021; NICE 2019).
Day‑by‑Day Timeline for D5 FET (DPT 1–14)
DPT 1–3: settling in; progesterone side‑effects
The embryo is in the cavity. It is not yet attached. Common feelings are bloating, fatigue, and mild cramps from progesterone support. Symptoms do not prove anything.
DPT 4–6: implantation window; what “twinges” may mean
Attachment and early invasion can start now. Some people notice light spotting. It can also be cervical irritation from progesterone. If bleeding is heavy or painful, call your clinic.
DPT 7–9: early hCG; why tests can still be negative
β‑hCG starts after implantation. Early urine tests can be negative even with a healthy pregnancy. False negatives are common before 9–11 DPT. Do not test multiple times per day.
DPT 10–11: reasonable home test timing
A sensitive test now has a better chance to detect hCG. First‑morning urine helps. If negative, wait 48 hours and try again. Bloods are more reliable.
DPT 12–14: stronger positives; when to book bloods
If pregnant, lines usually strengthen here. Book bloods with your clinic as advised. FET cycles typically have no hCG trigger interference.
Comment: What DPT are you on and did you test yet, or are you waiting for beta?
Symptoms vs Side‑Effects: What’s Normal vs Noise
Progesterone and oestrogen effects
Breast tenderness, bloating, nausea, mood changes, and sleep changes are common on progesterone and oestrogen. They are not proof of pregnancy.
Common symptoms that mean little
Mild cramps, back ache, extra hunger, or feeling warm can be medication or normal luteal phase. Track patterns, not single moments.
When symptoms matter
Severity, persistence, and red‑flag patterns matter more than single symptoms. If in doubt, call your clinic.
Evidence: Medication side‑effects can mimic early pregnancy. Rate‑of‑change in tests and ultrasound timing are more reliable (ACOG 2018; NICE 2019).
Testing Strategy After D5 FET
Earliest sensible home testing and why
After a D5 transfer, many services suggest waiting until at least 9–11 DPT before home testing. Earlier than that gives false negatives.
Blood beta timing; avoiding too‑early anxiety
Book bloods according to your service protocol. Testing too early only adds stress. FETs usually have no trigger shot to confuse results.
Mistake: testing multiple times per day
Use first‑morning urine. If negative, wait 48 hours. Then test again or follow your clinic’s plan.
Red Flags and When to Call Your Clinic
Urgent symptoms
Heavy bleeding, severe one‑sided pain, shoulder‑tip pain, faintness, or feeling very unwell. Seek urgent care.
Next steps your clinic may take
Repeat bloods and a timed transvaginal ultrasound once levels or dates make that useful.
Mistake: waiting days with severe symptoms
Do not wait. Call now. Services want to hear from you.
Evidence: NICE 2019 and RANZCOG 2023 advise urgent review for red‑flag symptoms or pregnancy of unknown location.
From Two‑Week Wait to First Scan
Typical timing after positive beta
Most services plan a first scan around 6–7 weeks. This is when a sac and yolk sac are likely to be seen.
What to expect at the scan
You may see a sac first, then yolk sac, then a fetal pole with cardiac activity. Timing varies.
Mistake: scanning too early
Too‑early scans often show little and increase worry. Follow your clinic’s timing.
Proof & Practicals
Mini case snapshot
A person tested at 8 DPT and got a negative. Tested again at 10 DPT and the line was clear. Bloods on 12 DPT confirmed pregnancy. Another person waited until 11 DPT for the first test and had one anxious day instead of three. Same outcome, less stress.
D5 FET DPT Windows at a Glance
| DPT window | What may be happening | Recommended action |
|---|---|---|
| 1–3 | Settling in; no reliable signals | Rest normal; do not over‑test |
| 4–6 | Possible implantation window | Note symptoms; call if heavy pain/bleeding |
| 7–9 | Early hCG begins | Avoid early tests or accept false negatives |
| 10–11 | Reasonable home test timing | Use first‑morning urine; retest in 48 h |
| 12–14 | Stronger positives if pregnant | Book bloods per clinic plan |
Checklist: if you plan to test
- Choose a sensitive brand and check expiry.
- Use first‑morning urine.
- If negative, wait 48 hours before testing again.
- Avoid testing many times per day.
- Keep notes; take a clear photo if needed.
- Book bloods with your clinic when advised.
- If anything feels wrong, call your clinic.
Myth vs Fact
Myth: More symptoms mean you are more likely pregnant.
Fact: Medication side‑effects and normal luteal changes often mimic pregnancy. Patterns and tests matter more.
Useful links
- When to test after FET — guidance on timing home pregnancy testing after frozen embryo transfer.
- Movement counting (kick counter tool) — interactive tracker for fetal movement (coming soon).
Sources (AU-focused)
- RANZCOG: Early pregnancy care (2023) — Royal Australian and New Zealand College of Obstetricians and Gynaecologists guideline.
- RACGP: Early pregnancy bleeding (2021) — clinical resource for Australian GPs.
- NICE: Ectopic pregnancy and miscarriage (2019) — UK guideline from the National Institute for Health and Care Excellence.
- ACOG: Early pregnancy loss (2018 update) — American College of Obstetricians and Gynecologists practice bulletin.
- Peer-reviewed reviews on implantation timing and early hCG kinetics (various years) — academic literature (multiple sources, journal-based).
FAQ
When does implantation happen after a D5 transfer?
Is spotting normal after embryo transfer?
Do cramps mean the embryo is implanting?
When should I use a home pregnancy test after D5 FET?
Can progesterone side‑effects mimic pregnancy?
What if I have no symptoms at all?
When should I call the clinic?
Conclusion
The best way to read embryo transfer day by day is to focus on DPT windows, not single symptoms. Wait for a sensible testing time. Plan bloods with your clinic. If something feels wrong, call. Calm and clear beats guesswork.
CTAs
- What DPT are you on—and did you test yet or are you waiting for beta? Share below.
- Bookmark this day‑by‑day guide and read our “When to test after FET” next.
Reminder: If you have heavy bleeding, severe pain, faintness, or shoulder‑tip pain, contact your fertility unit or emergency care.